Before going further, it’s worth pointing out that SARS-CoV-2 is neither malicious nor aware. It’s not capable of making plans. It doesn’t “want” anything. It is a quasi-living particle capable of reproduction with changes that are driven by a combination of random chance and selective pressure. To a large extent, that’s true for every living thing, but nowhere is it more true than with viruses.
In a 2013 paper, researchers from the University of Valencia said this: “RNA viruses are among the fastest mutating and evolving entities in nature.” SARS-CoV-2 is an RNA virus. Compared to a DNA virus like the variola virus behind smallpox, it changes more rapidly. And, in large part because the time of contact between human beings and SARS-CoV-2 is so brief, those changes can have significant effects.
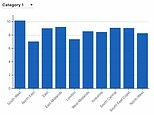
Here is a quick look at just one measure of how rapidly SARS-CoV-2 is changing.

In two years, SARS-CoV-2 has moved from being a virus with rate of infection that was roughly 50% greater than the flu, to one that matches up with the most infectious viruses known. There is no guarantee that this represents its upper bound. In fact, the drastic improvements seen from alpha to delta and delta to omicron suggests that there may be still quite a lot of “headroom” for SARS-CoV-2 on this single vector.
Of course, infectiousness isn’t everything. Smallpox is sitting back there at the bottom of the chart, barely twice as infectious as the flu, but no virus in history may be responsible for more human deaths than smallpox. In just the last 100 years before it was driven to extinction by a worldwide campaign of isolation and vaccination, smallpox accounted for an estimated 500 million deaths. That’s enough to cover everyone in the United States. And Canada. And Mexico. With another 10 million or so left over.
That’s because around 30% of people who caught smallpox died. For COVID-19, that number is around 1.2%. One person in 100 dying out of sight in a hospital is simply easier to overlook than a third of your family expiring after being consumed by pus-spewing sores.
Notice that there is no guarantee it will remain that way. The influenza virus—another of those pesky, rapidly changing RNA viruses—had been infecting humans for thousands of years before a version appeared in 1918 that greatly kicked up both the R0 and the mortality.
There’s nothing in any of these viruses driving them toward being significantly more lethal or significantly less lethal. Smallpox killed a high number of those infected, year in and year out, for thousands of years. If killing off a third of those infected had generated a significant selective pressure on the virus to be less lethal, you can bet the number would have dropped. It didn’t.
(Side note: For Ebola virus, increased lethality may actually be the result of selective pressure, as this virus is often transmitted by the handling of dead bodies.)
Right now, we’re still at the beginning of our relationship with SARS-CoV-2. We’ve already passed through a kind of Dunning–Kruger stage were we thought, or at least pretended, that we understood this virus and the disease it generates. We’re just starting to squeak past that to a point where we can admit our ignorance. We don’t know what kind of sequela are waiting for us years down the road. We’re only starting to become aware of horror stories like the one novapsyche covered in this diary.
A study from Tulane has come out that strongly suggests that, even in mild forms or onsets of the disease, even with asymptomatic presentation, the brain may experience diffuse yet profound insult in the form of “innumerable” microbleeds.
All of this just means that the idea that we should “just live with” COVID-19 and pretend that it doesn’t exist is an invitation to disaster of inestimable scale. That patient who tested positive over 505 days didn’t just have a persistent infection from SARS-CoV-2, they had a “unique” infection. Every single person infected generates unique infections, with genetic structures that are subtly different from the virus they had going in. If one of those unique versions happens to be more infectious, it stands a chance of being the next variant of concern, and what it does to us, from brain bleeds to death, barely matters.
It’s a race. And we can’t afford to stop running.